Qualitative testing is recommended in parallel with serum AAT testing and it is required for a definitive diagnosis of AATD.1 Qualitative testing includes phenotyping and genotyping.1
Phenotyping is performed to detect the most common AAT variants, including M, S, Z and null (no AAT synthesized) variants.1,7 In practice, phenotyping represents the genotype-by-proxy.8
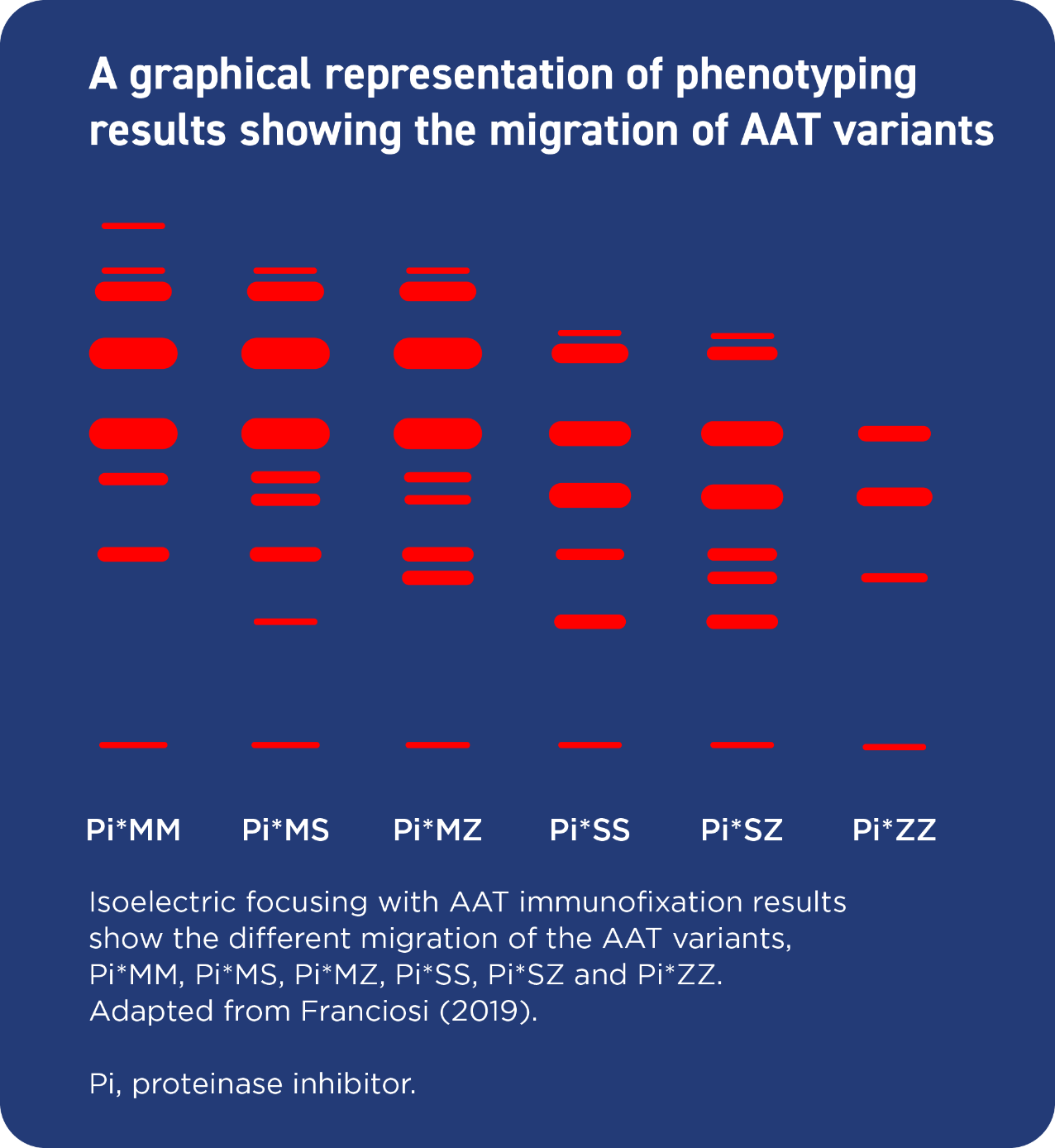
Phenotyping is performed on a serum or plasma sample using isoelectric focusing.1,3
Using the technique of electrophoresis, different AAT variants migrate at different rates through a polyacrylamide gel. The AAT variant present in a patient's sample can be determined based on the migration pattern; the Pi*Z variant migrates the slowest.3
Phenotyping allows the detection of heterozygosity.7
Individuals who are homozygous for the Z allele (Pi*ZZ) have a serum AAT concentration that is approximately 10-20% of levels reported in healthy individuals.3 The Pi*ZZ phenotype is present in 95% of individuals with clinical manifestations of AATD.3,9
Genotyping is used to determine mutations in the SERPINA1 gene and is performed at a molecular level using genomic DNA, which is extracted from circulating mononuclear blood cells.1,3,7
The genotyping technique most likely to be utilized is gene-targeted testing with polymerase chain reaction/denaturing gradient gel electrophoresis. This technique uses allele-specific probes for the S and Z variants to detect common pathogenic variants; however, rare variants such as the null variant can be missed.1,7,10
SERPINA1 gene sequencing can be performed if phenotyping and genotyping do not provide conclusive evidence of AATD, because it can detect uncommon AAT variants.7,8 The exome or whole genome can be sequenced to identify mutations.3,8